
Published by

Clinical Documentation as a Crisis: The Hidden Cost of Manual Note-Taking
The NHS faces one of its most persistent operational challenges: administrative burden. According to NHS Digital, clinicians currently spend between 40 and 50 per cent of their working hours on documentation and administrative tasks, rather than direct patient care. This inefficiency carries a devastating human cost. Documentation workload ranks among the top drivers of clinician burnout, directly contributing to the NHS's current shortage of more than 150,000 clinical staff.
For nurses, physicians, allied health professionals, and allied health providers, the relentless cycle of note-taking, coding, and administrative entry diverts focus from what drew them to medicine: patient interaction and clinical decision-making. The burden extends beyond frustration. Poor documentation practices increase medical errors, create compliance risk, delay patient handovers, and slow revenue cycle management. In some cases, clinical information is transcribed multiple times across different systems, each entry a point of human error and a drain on finite clinical time.
Artificial intelligence offers a direct, measurable solution to this crisis. Ambient listening systems, speech-to-text engines, and automated coding platforms are fundamentally reshaping how healthcare organisations manage documentation. Rather than replacing clinicians, these technologies restore time and accuracy—freeing clinicians to focus on what matters most: patients.
Understanding Ambient Clinical Documentation and AI-Powered Listening
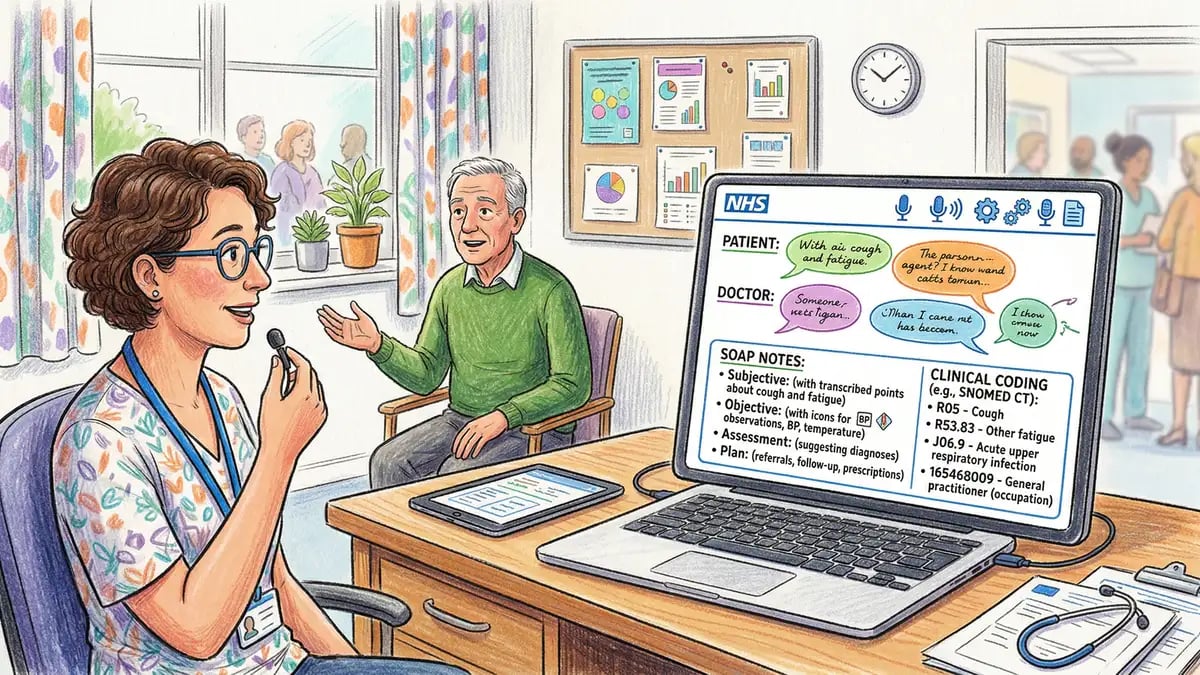
Ambient clinical documentation represents a paradigm shift in how healthcare notes are created. Instead of stopping mid-consultation to type, dictate, or document after a patient encounter, ambient listening systems continuously record clinical conversations and automatically generate structured notes in real time or within seconds of the encounter.
The technology works through several integrated components. Natural language processing (NLP) engines listen to clinician-patient dialogue, identifying key clinical concepts, diagnoses, medications, and procedural details. Machine learning models trained on millions of de-identified patient records recognise clinical context, flagging important findings and translating spoken language into standardised medical terminology. These systems integrate directly with electronic patient records (EPRs), clinical decision support systems, and billing workflows, eliminating manual transcription and entry.
Organisations deploying ambient clinical documentation report transformative results. Clinicians save 1 to 3 hours per day on documentation alone. A discharge summary—traditionally requiring 15 to 30 minutes of manual work—can be generated and reviewed in minutes. Real-time documentation ensures more complete, accurate records at the point of care, improving both clinical safety and audit compliance.
For healthcare providers operating under severe time pressure, this reclaimed time translates directly into capacity: more patient consultations, fewer overtime hours, and improved clinician wellbeing.
Accuracy and Coding: Where AI Outperforms Manual Documentation
One of the most compelling business cases for AI-powered documentation lies in medical coding accuracy. Accurate coding is critical for three reasons: clinical safety (diagnoses and procedures must be recorded correctly for continuity of care), compliance (incorrect coding can trigger audits and sanctions), and revenue (the NHS and private providers depend on coding accuracy for appropriate reimbursement and commissioning).
Manual coding by human coders achieves 80 to 85 per cent accuracy against gold-standard datasets. AI systems using deep learning models trained on hundreds of thousands of coded records achieve 95 per cent or higher accuracy for ICD-10 and SNOMED CT classifications. This precision difference is not trivial. For every 100 patient records, AI reduces coding errors by 10 to 15 cases, minimising compliance risk and improving revenue capture by 5 to 15 per cent.
The accuracy advantage stems from AI's ability to cross-reference clinical text against standardised terminology in milliseconds, avoid fatigue-related mistakes (coding is mentally taxing), and apply consistent rules across millions of records without exception. Clinical teams can review AI suggestions and override when needed—a hybrid model that combines machine speed with human clinical judgement.
Real-World Deployments: Ambient AI Across UK and International Healthcare
Ambient clinical documentation is no longer experimental. Across the UK and internationally, healthcare organisations are scaling these systems with measurable results.
Dragon Medical One, developed by Nuance (now part of Microsoft), has been deployed across more than 200 NHS trusts and private healthcare providers. It combines speech recognition with clinical-specific vocabulary, allowing clinicians to dictate notes naturally whilst the system translates speech into structured EHR entries. The system learns individual clinician speech patterns over time, improving accuracy and reducing correction time.
Nuance DAX (Digital Ambient Experience) represents a next-generation approach, combining ambient listening with real-time clinical intelligence. The system listens passively to clinician-patient conversations, identifies clinical documentation opportunities, and suggests relevant findings, diagnostics, and treatment options in real time. Several UK hospital systems have piloted DAX within their emergency departments and acute wards, reporting rapid adoption and high clinician satisfaction.
Augnito, a UK-developed speech-to-text platform designed specifically for clinicians, offers cloud-based ambient listening with integration into major EPR systems used across the NHS. The platform emphasises data privacy and compliance, holding data within UK data centres and complying with NHS Data Security and Protection Toolkit requirements.
Beyond the UK, healthcare systems in the United States, Australia, and Canada have reported substantial benefits: average documentation time reduction of 50 to 60 per cent, improved coding accuracy, and clinician satisfaction scores above 85 per cent after a brief adoption period.
Integration with NHS Digital Infrastructure and Interoperability Standards
Successful implementation of AI documentation systems depends on deep integration with existing NHS digital infrastructure. The NHS is undergoing substantial digital transformation, driven by the Digital Maturity Assessment and the NHS England Long Term Plan commitment to reduce administrative burden and improve digital capability.
Most modern EPR systems—including EPIC, Cerner, and Allscripts—now offer native integrations or API-based connections for ambient documentation and speech-to-text services. The HL7 FHIR (Fast Healthcare Interoperability Resources) standard is becoming the de facto interoperability framework for NHS organisations, enabling ambient documentation systems to read clinical context from multiple legacy systems and write structured data back to EPRs seamlessly.
This standardisation matters enormously. Rather than custom integration work for each hospital, vendors can deploy ambient documentation systems rapidly across multiple trusts using standardised APIs. Clinicians moving between hospitals experience consistent documentation workflows, reducing training time and accelerating adoption.
NHS Digital's governance framework also sets clear expectations: AI documentation systems must be auditable, maintain full clinical accountability (meaning clinicians remain responsible for accuracy), provide clear evidence trails, and comply with data protection and information governance standards. Forward-thinking healthcare organisations are embedding these requirements into procurement and implementation from day one, ensuring AI systems enhance rather than undermine trust and safety.
Clinical Governance and Accountability in AI-Generated Documentation
A critical question emerges as AI documentation becomes mainstream: who is responsible if an AI system generates an incorrect or incomplete note? The answer, according to General Medical Council (GMC) guidance, is unambiguous: the clinician remains accountable.
This principle underpins the safe adoption of AI documentation. Clinicians are responsible for reviewing AI-generated notes before finalisation, correcting errors, and ensuring the record accurately reflects the clinical encounter. In practice, most organisations implement a review workflow where AI generates a draft note within seconds, the clinician reviews and edits (if needed) within the encounter or shortly after, and the finalised note is signed off in the EPR.
This human-in-the-loop approach yields several benefits. Clinicians maintain clinical oversight and accountability. Audit trails show who reviewed and approved each note, protecting both the clinician and the organisation. AI systems can be refined over time based on correction patterns, gradually improving accuracy and reducing review time. And crucially, clinicians remain confident in the system because they understand how it works and retain control.
Nursing and Midwifery Council (NMC) guidance mirrors this principle, emphasising that nurses must be able to explain and justify all entries in the patient record, regardless of whether AI assisted in generating them. Professional bodies across healthcare—from radiologists to physiotherapists—are converging on the same conclusion: AI is a powerful tool, but clinical professionals must remain the final decision-maker.
Revenue Cycle Optimisation: Medical Coding and Billing Efficiency
Beyond clinical efficiency, AI documentation systems deliver substantial financial benefits through improved medical coding and billing workflows. Every hospital and healthcare provider manages thousands of patient episodes per month, each generating billing codes that determine reimbursement from commissioners, insurance companies, or patients.
Manual coding introduces systematic losses. Coders working under time pressure may miss secondary diagnoses or complications, leading to under-coding (receiving payment for only the primary procedure rather than all relevant services rendered). Incomplete coding also distorts performance metrics, making it difficult for services to justify staffing or investment. By contrast, AI-powered coding systems systematically extract all clinical information from notes, ensuring comprehensive coding and maximising appropriate reimbursement.
The financial impact is measurable. Healthcare organisations implementing AI-assisted coding report improved revenue capture of 5 to 15 per cent on the same volume of patient activity. For a 400-bed hospital performing 10,000 procedures annually at an average value of £5,000 per coded episode, a 10 per cent improvement in coding completeness translates to £5 million in additional annual revenue. Even accounting for implementation costs, the return on investment is typically achieved within 12 to 18 months.
Beyond coding accuracy, AI documentation systems reduce billing delays. Traditional workflows involve documentation → manual transcription → coding → billing, with days or weeks between clinical encounter and claim submission. Ambient documentation systems compress this to documentation → review → coding → billing within hours, accelerating cash flow and reducing working capital requirements.
Discharge Summaries and Continuity of Care
Discharge summaries represent a critical but time-consuming component of clinical documentation. A comprehensive discharge summary must include admission reason, clinical course, findings, procedures, medications, and follow-up instructions—all synthesised from multiple clinical notes, investigations, and conversations.
Manually generating a discharge summary typically requires 15 to 30 minutes of clinician time, often completed at the end of a shift when cognitive load is highest and accuracy is compromised. Delays in discharge summary production impair continuity of care. General practitioners may not receive discharge summaries for weeks after a patient returns home, preventing timely medication adjustments or follow-up investigations. This gap in information is a known risk factor for readmission and adverse events.
AI systems specifically trained on discharge summary templates can generate comprehensive summaries from ambient documentation in minutes. The summary includes all required elements, follows standard formatting for legibility, and is ready for clinician review and sign-off. Early adopters report that this automation reduces the time to discharge summary generation from hours to minutes, improves information completeness, and accelerates GP notification—ultimately improving patient safety and reducing preventable readmissions.
Clinician Adoption: User Experience and Change Management
The most powerful technology fails without clinician adoption. Fortunately, ambient documentation systems have been refined through thousands of implementations, and user experience is increasingly a design priority.
Modern ambient systems are designed to be passive and unobtrusive. Unlike traditional voice recognition systems that require conscious dictation, ambient listening works naturally within existing consultation workflows. Clinicians do not need to change their behaviour, speak into a specific microphone, or use a separate interface. They simply consult as usual whilst the system listens and generates notes in the background.
Adoption rates reflect this user-friendliness. Early-stage deployments in UK hospitals report that 70 to 85 per cent of clinicians adopt ambient documentation within 2 to 4 weeks of availability, often without formal training. Those who initially resist typically convert after observing colleagues' time savings. Many organisations find that adoption accelerates when clinicians see not just saved time but improved note quality and reduced dictation burden.
Implementation success depends on thoughtful change management. Organisations that involve clinician champions early in vendor selection, pilot new systems in engaged teams before broader rollout, and provide accessible technical support report substantially higher adoption rates and faster time-to-value. Conversely, organisations that impose systems top-down without clinical input often encounter resistance and slower realisation of benefits.
Data Privacy, Security, and Compliance in Healthcare AI
Healthcare data is among the most sensitive information organisations manage. Ambient documentation systems record voice data (patient conversations), process clinical information in real time, and store conversations and derivatives. This creates rigorous data governance requirements.
Leading vendors address these requirements through several mechanisms. Many systems offer on-premise or UK-hosted deployment options, ensuring patient data never leaves NHS infrastructure. End-to-end encryption protects data in transit. Advanced access controls and audit logging track who accesses what data. De-identification capabilities allow organisations to use real clinical data for system training and improvement without exposing patient identities.
Compliance with UK data protection law (UK GDPR and the Data Protection Act 2018) is non-negotiable. Healthcare organisations must conduct Data Protection Impact Assessments (DPIAs) before deploying any AI system that processes patient data. Information Commissioner's Office (ICO) guidance emphasises that organisations remain responsible for ensuring AI systems process personal data fairly, transparently, and lawfully.
NHS trusts implementing ambient documentation increasingly embed data governance into procurement, requiring vendors to demonstrate GDPR compliance, data residency options, and third-party security assessments before contract signature. This rigorous approach takes longer upfront but prevents downstream legal and ethical complications.
Implementing AI Documentation: A Practical Roadmap for Healthcare Organisations
Successful implementation of AI documentation systems follows a predictable pattern, tested across hundreds of healthcare organisations globally.
Phase 1: Assessment and Planning (4 to 6 weeks). Organisations assess current documentation workflows, identify pain points, and define success metrics (time savings, coding accuracy, clinician satisfaction, revenue impact). Clinical and IT teams align on requirements, including EPR integration, interoperability standards, and compliance expectations. Vendor shortlisting begins, with evaluation criteria reflecting organisational priorities.
Phase 2: Pilot and Proof of Concept (8 to 12 weeks). A small group of engaged clinicians (typically 10 to 30) use the selected system in a real clinical environment. The pilot is structured: clinicians document normally, the system generates draft notes, clinicians review and correct, and feedback is collected. Metrics are measured weekly. This phase de-risks the investment and generates clinician testimonials for broader rollout.
Phase 3: System Configuration and Training (4 to 8 weeks). If the pilot is successful, the system is configured to match organisational standards: dictation templates, coding rules, alert triggers, and integration with existing EPRs and workflows. Clinical staff and IT teams receive training. Documentation is prepared: policies on clinical accountability, audit trail requirements, and exception handling.
Phase 4: Rollout and Scale (8 to 16 weeks). The system is deployed to target departments or teams in waves. Each wave includes technical support, quick-reference guides, and regular feedback sessions. Metrics are tracked continuously. As clinicians gain confidence, adoption typically accelerates. Most organisations achieve >80 per cent usage within 12 weeks of rollout in target areas.
Phase 5: Optimisation and Continuous Improvement. As adoption stabilises, organisations refine the system: adjusting templates based on clinician feedback, retraining AI models on real organisational data to improve accuracy, integrating additional workflows (e.g., prior authorisation, referral letters), and measuring long-term impact on clinical outcomes, patient safety, and organisational efficiency.
Measuring Impact: Quantifying the Benefits of AI Documentation
Healthcare leaders rightly expect evidence that investment in AI documentation delivers tangible value. Fortunately, impact is measurable across multiple dimensions.
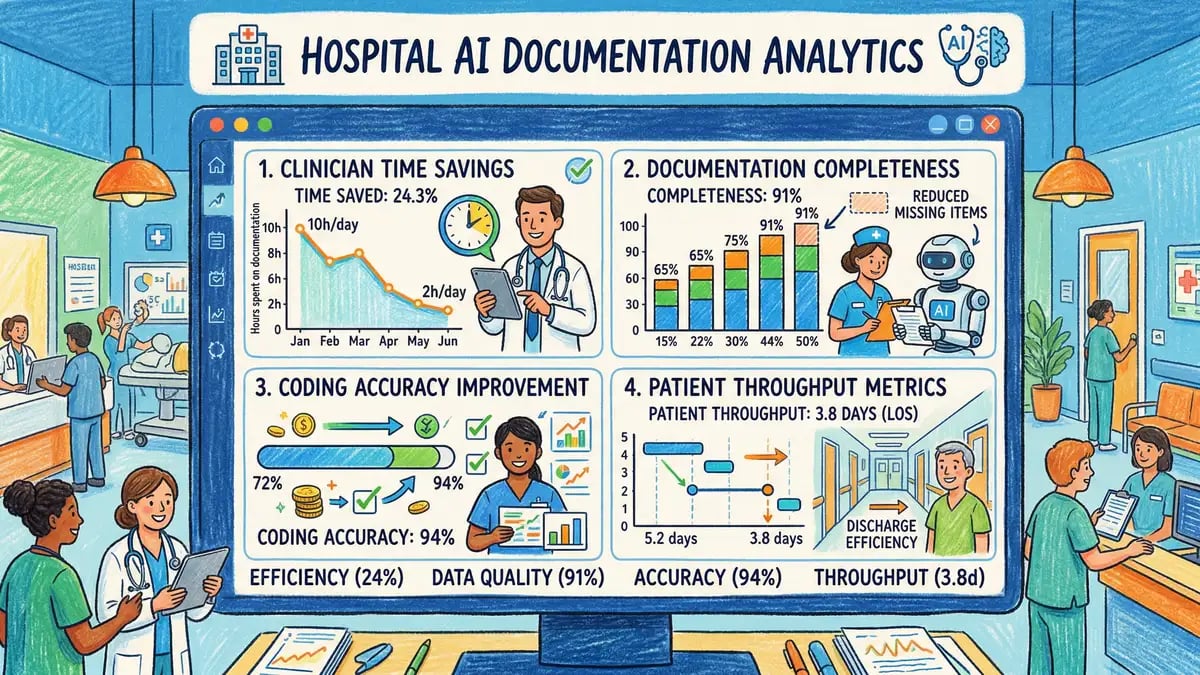
Clinician Time. Time studies conducted before and after implementation consistently show 1 to 3 hours of daily time savings per clinician. In some specialties (e.g., emergency medicine, intensive care, acute admission units), savings approach 3 hours per day. This time is reinvested in patient care, clinical teaching, or administration—whatever the organisation prioritises.
Documentation Completeness. Chart audits comparing pre- and post-implementation documentation show substantial improvements in note completeness, with documented clinical findings increasing by 20 to 40 per cent. This reflects both the ambient system's ability to capture information clinicians might previously have omitted under time pressure, and improved coding that emerges from more complete documentation.
Coding Accuracy. Blind audits of AI-coded cases versus manual coding show AI accuracy of 95 per cent or higher, compared with 80 to 85 per cent for manual coding. The accuracy advantage is consistent across coding categories.
Revenue Cycle Metrics. Organisations track days from discharge to billing, coding completeness (number of billable codes per episode), and reimbursement realisation rates. Implementations typically show 5 to 15 per cent improvements in revenue metrics, translating to millions of pounds annually for large healthcare providers.
Clinician Satisfaction and Retention. Post-implementation surveys consistently show high clinician satisfaction (typically >80 per cent would recommend the system to colleagues). Over longer timescales, healthcare organisations see improvements in clinician retention, reduced locum costs, and improved staff morale in departments using ambient documentation.
Patient Safety Metrics. Whilst randomised controlled trials are limited, observational data from large implementations shows associations between better documentation (enabled by ambient systems) and improvements in clinical safety metrics: reduced medication errors, faster response to critical findings, and improved adverse event detection.
Overcoming Implementation Challenges and Resistance
Despite the compelling business case, healthcare organisations implementing AI documentation often encounter predictable challenges.
Technical Integration Complexity. Legacy EPR systems may lack APIs or modern integration capabilities. Solution: involve IT early in vendor selection, ensure vendors commit to integration support, and consider whether a phased rollout (starting with departments using modern EPRs) is more realistic than organisation-wide implementation.
Clinical Resistance. Some clinicians distrust AI or fear job displacement (particularly for medical coders). Solution: engage clinical champions early, provide transparent communication about how AI augments rather than replaces human judgement, emphasise time savings and improved work environment, and ensure clinicians maintain full control over finalised documentation.
Data Governance and Compliance. Organisations often underestimate the time required for data protection assessments, compliance reviews, and governance sign-off. Solution: begin governance discussions during vendor evaluation, involve information governance, legal, and clinical audit teams early, and plan realistic timelines (typically 8 to 12 weeks for comprehensive compliance assessment).
Change Management Fatigue. Healthcare staff are often overwhelmed with ongoing system implementations and training demands. Solution: position AI documentation as a burden-reduction initiative (not another task), provide practical support (guides, champions, dedicated helpline), and celebrate early wins to build momentum.
Future Directions: Generative AI and Predictive Clinical Insights
Ambient clinical documentation has already transformed healthcare note-taking. Emerging developments promise even greater impact.
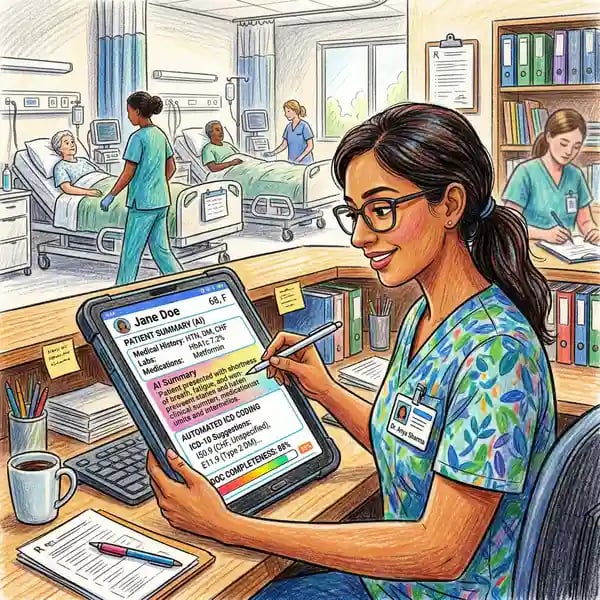
Generative Language Models. Newer systems employ large language models (LLMs) fine-tuned on medical literature and de-identified clinical records. These models can generate not just transcriptions of clinical conversations, but comprehensive clinical summaries, risk assessments, and recommended follow-up actions based on the entire clinical context.
Real-Time Clinical Decision Support. Advanced systems integrate documentation with clinical decision support, flagging relevant protocols, evidence-based guidelines, and safety alerts during the encounter. This moves AI from a documentation tool to a clinical reasoning assistant, improving diagnosis and treatment decisions in real time.
Predictive Analytics. By combining documented clinical information with historical outcomes data, AI systems can identify patients at high risk of adverse events, readmission, or poor outcomes, enabling proactive intervention before crisis occurs.
Cross-Organisational Learning. Federated learning approaches allow multiple healthcare organisations to train shared AI models on real clinical data whilst maintaining patient privacy and data security. This accelerates model improvement and enables smaller organisations to benefit from insights derived from millions of encounters across the NHS.
Frequently Asked Questions: Clinical Documentation AI in Healthcare
What happens if an AI documentation system generates an incorrect note?
The clinician remains responsible for all documentation in the patient record. In practice, clinicians review AI-generated notes before finalisation, correcting errors or omissions. This human-in-the-loop approach ensures accuracy whilst leveraging AI's speed and consistency. Most implementations report that initial notes require corrections in only 10 to 20 per cent of cases, and correction time is minimal because the AI has already captured the clinical narrative.
Are patient conversations stored indefinitely? What are the data privacy implications?
Leading vendors store voice recordings only as long as necessary for documentation and quality assurance, typically 30 to 90 days. Organisations control data retention and can specify shorter retention periods if desired. Many vendors offer deployment options where data remains within NHS infrastructure, ensuring compliance with UK GDPR. Healthcare organisations must conduct Data Protection Impact Assessments before deployment, ensuring vendors meet all compliance requirements.
How much does ambient clinical documentation cost, and what is the payback period?
Costs vary by vendor, deployment model, and organisational size, typically ranging from £5,000 to £25,000 per clinical user per year. Larger organisations negotiate volume discounts. Payback periods are rapid: organisations typically recover implementation costs within 12 to 18 months through improved coding accuracy, revenue capture, and clinician time savings. For large providers, the financial case is compelling: reclaimed clinician time alone often justifies the investment.
Will AI documentation systems replace medical coders?
No. Instead, AI shifts coders' role from manual data entry to quality assurance and exception handling. As AI handles routine coding, coders focus on complex cases, unusual presentations, and ensuring coding completeness and compliance. Many organisations find that AI allows them to expand coding coverage (improving revenue capture) without proportional increases in coding staff.
How long does it take to implement ambient documentation across a healthcare organisation?
Typical timelines are 6 to 12 months from vendor selection to full rollout, depending on organisational size and complexity. Pilot phases take 8 to 12 weeks, configuration and training take 4 to 8 weeks, and departmental rollout takes 8 to 16 weeks. Smaller organisations or those with modern, integrated EPR systems can often accelerate these timelines.
Related Reading and Further Exploration
AI documentation is part of a broader transformation in healthcare intelligence and automation. For deeper exploration of related topics, explore our guides on AI for healthcare delivery, AI for pharmaceutical discovery, AI for medical imaging and diagnostics, and AI for mental health care. Healthcare compliance and governance are critical, as detailed in our resource on AI compliance in healthcare. For sector-specific insights, explore our guides on AI for dentistry and AI for pharmacy operations. For organisations ready to move beyond single-function tools toward integrated AI capability, our guide to AI training for healthcare professionals offers a structured pathway.
Ready to Transform Clinical Documentation with AI?
Helium42 helps healthcare organisations build internal AI capability through education-led implementation. From ambient documentation to medical coding, our programmes deliver measurable results in 6 to 8 weeks. Our team works alongside your clinical and IT leaders to assess current workflows, design implementation roadmaps, and ensure AI systems integrate seamlessly into your existing practices. With successful deployments across 500+ companies, 2,000+ professionals trained, and 200+ workshops delivered globally, we understand healthcare's unique challenges and opportunities.
Book a Consultation

