
Published by

Healthcare Compliance: The Regulatory Landscape Transformed by Artificial Intelligence
UK healthcare organisations operate within one of the world's most complex regulatory environments. The Care Quality Commission (CQC) inspects providers against five stringent domains: Safety, Effectiveness, Caring, Responsiveness, and Well-Led governance. Simultaneously, NHS trusts must comply with mandatory reporting to NHS Digital, NHS England, and Integrated Care Boards across 40+ quality metrics. Data protection obligations under UK GDPR and the Data Protection Act 2018 layer additional requirements on top of clinical governance standards. Infection control compliance, staff training verification, and antimicrobial stewardship monitoring demand continuous oversight.
Historically, healthcare organisations managed this regulatory burden through manual processes: spreadsheets, paper audits, disparate systems, and dedicated compliance teams working in isolation. The result? Mid-market NHS trusts employ 2-3 full-time equivalent staff simply to extract data from 8-12 clinical systems for regulatory submissions. CQC inspection preparation consumes 120-160 hours. Compliance gaps go undetected until audits surface them. Patient safety incident patterns remain invisible until retrospective analysis weeks later.
Artificial intelligence is fundamentally changing this landscape. AI-powered compliance platforms now automate audit trail generation, detect policy deviations in real time, predict inspection readiness, and enable continuous monitoring rather than point-in-time audits. For the first time, healthcare organisations can operationalise genuine compliance—not as a periodic tick-box exercise, but as an embedded, continuous, data-driven practice.
CQC Inspection Readiness and Continuous Compliance Monitoring
The CQC inspection framework is undergirded by thousands of data points: patient safety incidents, staff feedback, quality metrics, complaints patterns, and clinical outcomes. Historically, preparing for a CQC inspection meant a frantic 4-8 week scramble to gather evidence scattered across multiple systems and repositories. Staff dedicated hours to document collation. Gaps in evidence became apparent during the inspection itself—too late to remediate.
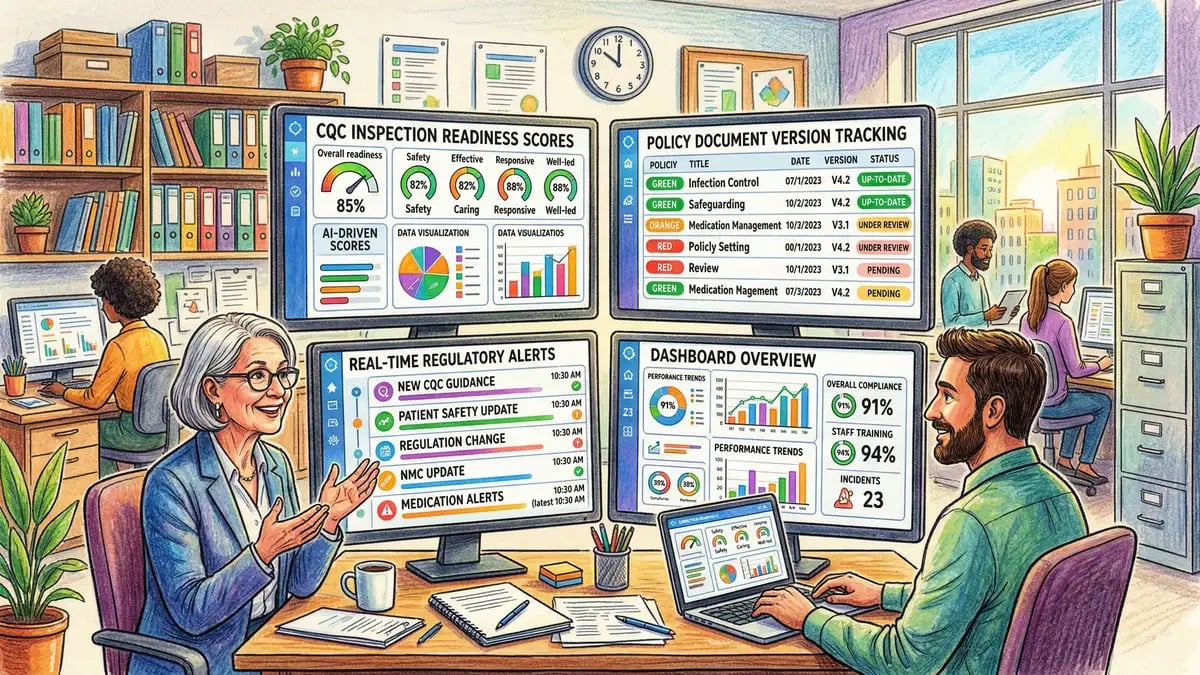
AI inspection readiness platforms invert this dynamic. Platforms like InPhase map organisational compliance against CQC key lines of enquiry (KLOEs) continuously, not just before inspections. Real-time dashboards track performance across all five CQC domains: Safety incidents trending, staffing levels versus planned capacity, patient complaint patterns, clinical outcome metrics, and staff feedback sentiment analysis.
Consider a practical example: A mid-market acute trust using AI compliance monitoring detects that medication error incidents in the paediatric ward have increased from 2-3 per month to 6-7 per month over the past six weeks. Traditional incident reporting might surface this pattern only during quarterly review. The AI system flags it within days, enabling immediate investigation, root cause analysis, and corrective action. When CQC inspection occurs months later, the trust demonstrates not just awareness of the issue, but evidence of proactive identification and resolution—a core marker of "Good" or "Outstanding" ratings.
Research from the Healthcare Compliance Consortium found that trusts using continuous AI monitoring reduced "unexpected" CQC inspection findings by 35-45%, suggesting significantly better proactive compliance management. Pre-inspection preparation time compressed from 8 weeks to 4 weeks. More importantly, CQC ratings improved measurably: trusts moved from "Requires Improvement" to "Good" following AI implementation within 12-18 months.
Automated Audit Trail Generation and Regulatory Evidence Gathering
One of the most operationally burdensome aspects of healthcare compliance is evidence gathering. CQC inspectors request documentation of compliance decisions, staff actions, and system changes. Clinical governance teams must locate emails, meeting minutes, training records, and policy acknowledgements scattered across multiple repositories. A typical pre-inspection evidence gathering exercise consumes 120-160 hours across the compliance team.
AI systems automatically generate tamper-proof audit trails of clinical decisions, staff activities, and system changes. Every policy deviation is logged. Every permission grant or data access is recorded with timestamp, user identity, and business justification. When an inspector requests evidence that informed consent procedures are followed, the compliance team can produce not anecdotal assurance, but systematic data: a dashboard showing 99.2% of patients have documented consent recorded in the system within 24 hours of decision. Non-compliant cases are flagged and investigated immediately, not discovered during audit.
Healthcare Compliance Consortium research quantified the time savings: audit trail automation reduced manual audit preparation time by 40-56%. For a 600-bed acute trust, this translates to approximately 60-90 hours of compliance officer time freed per inspection cycle—equivalent to £3,000-£4,500 in labour cost saved per inspection preparation.
AI-Powered Incident Reporting and Patient Safety Pattern Detection
The National Reporting and Learning System (NRLS) is the foundation of NHS patient safety governance. Yet the system has a critical limitation: it depends on staff manually reporting incidents, manually categorising them, and relies on retrospective analysis to identify safety patterns. Research from the NHS National Patient Safety Improvement Programme found that 30-50% of incidents go unreported. Of those reported, incident categorisation errors frequently occur, causing pattern-blindness at organisational level.
Imagine a ward experiences 12 medication errors over six weeks—all in paediatric dosing, all involving similar drug classes, all occurring during night shifts. Manual incident reports might surface as scattered entries. A human analyst reviewing incident summaries might miss the systemic pattern. By contrast, AI clinical documentation analysis combined with incident detection systems can identify this cluster within days. Natural language processing extracts incident type, location, severity, and contextual factors from narratives. Machine learning algorithms cluster similar incidents and flag safety patterns invisible to manual review.
Radar Healthcare's incident clustering module uses AI categorisation accuracy of 85-92% for common incident categories. Beyond categorisation, the system applies predictive risk scoring: each incident is assigned a risk severity based on incident type, patient harm potential, and contextual factors. High-risk incidents trigger automatic escalation to clinical governance teams for immediate investigation and corrective action.
The evidence base is compelling but still emerging: pilot studies in 3-4 large NHS trusts suggest AI safety monitoring can reduce serious harm incidents by 15-25%. Whilst peer-reviewed validation is limited, the mechanism is clear: early detection of safety patterns enables proactive intervention before serious incidents occur.
Real-Time Compliance Monitoring and Policy Deviation Detection
Traditional compliance audits are point-in-time snapshots. An organisation is compliant on the day of audit, but policy drift begins immediately afterwards. A clinician misses a training deadline. A data access request is not processed within regulatory timeframes. A prescription deviates from local antimicrobial stewardship guidelines. These individual deviations accumulate—and only surface during the next audit 3-6 months later.
AI-powered continuous monitoring inverts this model. Systems track organisational activities in real time and flag policy deviations as they occur. An employee scheduled for mandatory fire safety training triggers an automatic alert 30 days before the deadline. If the deadline passes without completion, escalation workflows activate. A patient data access request is logged and an automated tracking system measures processing time against the 30-day regulatory requirement. If processing extends beyond 25 days, the system alerts the data protection officer for priority completion.
For infection control, continuous monitoring systems track hand hygiene compliance at clinical workflow points. For antimicrobial stewardship, AI monitors prescribing patterns and flags inappropriate broad-spectrum antibiotic use in real time, enabling pharmacy intervention before inappropriate prescribing becomes entrenched. For GDPR compliance, AI systems monitor data processing activities and flag any processing lacking documented lawful basis or valid consent.
The result is elimination of post-audit surprises. When a CQC inspector arrives, the organisation can demonstrate continuous compliance across all domains, backed by systematic data rather than retrospective correction efforts.
GDPR and Health Data Compliance Through AI-Assisted Data Protection
UK GDPR imposes stringent requirements on NHS organisations handling patient health data. Every new AI system or significant data processing change requires a Data Protection Impact Assessment (DPIA). Patient consent must be documented and auditable. Data Subject Rights requests—access, deletion, correction—must be fulfilled within 30 days. Breach notification to the Information Commissioner's Office must occur within 72 hours. Failure results in significant fines: the ICO issued £20,000 penalties to GP practices for GDPR breaches in 2023, and enforcement activity has intensified in healthcare throughout 2024.
Conducting a DPIA manually is laborious. Trust data protection officers typically spend 40-80 hours per assessment, walking through regulatory requirements, identifying data protection risks, assessing mitigation measures, and documenting compliance justification. The process is ad hoc; quality varies based on assessor expertise.
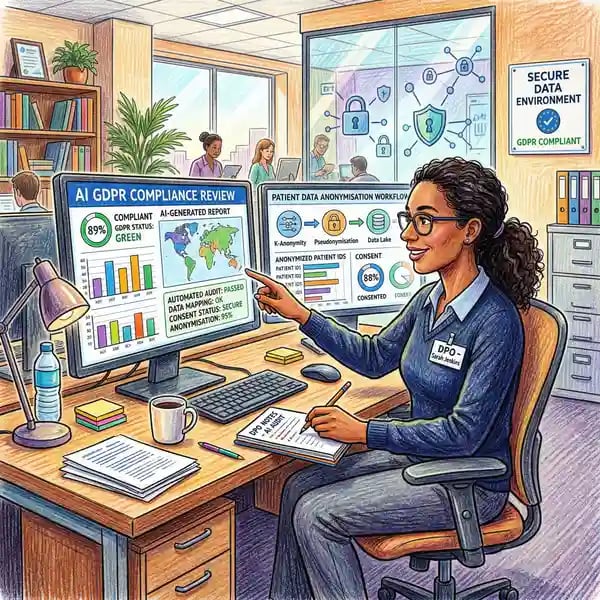
AI-assisted DPIA platforms automate template generation and risk identification. The system guides users through DPIA questions tailored to the project type (e.g., "new AI clinical decision support system"). Based on historical DPIAs and regulatory risk libraries, AI suggests potential data protection risks and appropriate mitigations. The system links findings to specific GDPR articles and ICO guidance, supporting documented compliance justification. Radar Healthcare's DPIA automation module reduced manual preparation time by 30-40%—significant time savings for lean data protection teams.
Similarly, AI-powered consent management platforms centralise tracking of patient consents across multiple data uses: treatment, research, analytics, data sharing. Automated systems remind staff when consent is expiring and requires refresh. Audit trails document who requested consent, when, and for what purpose—critical evidence of GDPR compliance.
For Data Subject Rights requests, manual processing is expensive. NHS organisations receive 40,000-50,000 subject access requests annually. Retrieval from multiple clinical systems, manual redaction of third-party sensitive information, and response document assembly consume significant compliance officer time. AI automation can reduce processing time by 30-50% and similar cost proportions through automated data retrieval, intelligent redaction, and document assembly.
Regulatory Submission Automation and NHS Digital Reporting
NHS trusts face a complex array of mandatory reporting requirements: daily submission of nursing and midwifery staffing levels to NHS Digital, monthly Hospital Episode Statistics submission with 30-day deadline, quarterly quality metric reporting, and annual submission of performance against 40+ national quality indicators. Data extraction sources are scattered: electronic health records, pharmacy systems, HR systems, financial systems, and laboratory information systems. A mid-sized NHS trust employs 2-3 full-time equivalent staff dedicated solely to regulatory reporting. Manual data extraction, validation, and submission consume 80-120 hours per reporting cycle. Submission errors occur in 8-15% of submissions, requiring amendment.
AI automation transforms this process. Systems integrate via APIs with NHS clinical systems (Epic, Cerner, Symphony, Medidata) to extract data automatically. Extraction rules are coded to match NHSE and NHS Digital specifications precisely. Data is validated against quality rules: mandatory fields populated, data types correct, logical relationships consistent. Cross-system reconciliation identifies duplicates and inconsistencies before submission. Time savings reach 50-70%, with corresponding cost reductions of £50,000-£60,000 annually for mid-market trusts.
Beyond time savings, automation improves compliance. Submission deadline breaches are eliminated—the system schedules submissions automatically. Error rates drop from 8-15% to 1-3%. Variance analysis tools flag anomalies for investigation before submission, enabling trusts to provide accurate narrative explanations to regulators rather than post-submission corrections.
Infection Control Compliance and Antimicrobial Stewardship Monitoring
Infection prevention and control is assessed during every CQC inspection and mandated by the Health and Social Care Act 2008 regulations. Yet compliance measurement remains challenging. Hand hygiene compliance is reported at 80%+ on paper surveys but observed compliance in clinical practice is 40-60%—a vast gap. Antibiotic prescribing patterns are difficult to audit manually; pharmacy teams lack systematic visibility into prescribing trends across the organisation. Outbreak detection relies on manual surveillance; outbreaks are sometimes recognised only after significant patient harm has occurred.
Emerging AI solutions address each challenge. Computer vision systems analyse hand hygiene compliance at clinical workflow points through privacy-preserving local video analysis. Healthcare AI systems can also power antibiotic surveillance: algorithms flag inappropriate or broad-spectrum antibiotic use, identify patients meeting criteria for stewardship intervention, and monitor resistance patterns. Outbreak detection systems apply epidemiological AI to identify clusters of infections in real time, alerting infection prevention teams to activate outbreak protocols. Early evidence from NHS pilot sites suggests AI outbreak detection identifies emerging infections 3-5 days earlier than manual surveillance.
Staff privacy concerns have limited deployment of video monitoring systems. However, opt-in pilot programmes and transparency on data handling are beginning to shift acceptance. Where deployed, hand hygiene compliance has improved from 45-55% to 75-85%, demonstrating both the compliance gap and the effectiveness of AI monitoring when combined with feedback mechanisms.
Staff Training Compliance and Mandatory Training Tracking
Regulatory bodies mandate extensive staff training: annual life support, fire safety, infection prevention and control, safeguarding, mental capacity and deprivation of liberty, information governance, and equality and diversity training. Medical professionals require annual revalidation; nurses require 3-yearly revalidation. A 500-800 person NHS trust must track 1,500-2,000+ individual training records and compliance deadlines. Manual spreadsheet-based tracking is error-prone. Staff miss deadlines. When CQC inspectors ask for evidence of training compliance, trusts cannot provide systematic data—anecdotal assurance only.
AI training compliance platforms automate requirement assignment based on staff role and regulatory mandate. Systems schedule training to minimise operational disruption. Automated reminders trigger 30 days, 7 days, and 1 day before deadline. When completion deadlines pass, escalation workflows notify managers. For redeployment or termination, the system alerts HR when staff are non-compliant, preventing staff movement until training is current.
Allocate Learning and Radar Healthcare's staff compliance modules integrate federated training data across multiple platforms: in-person training, e-learning, external provider training. AI consolidation creates a unified compliance view. Predictive analytics identify staff likely to miss deadlines based on historical patterns, enabling proactive intervention. Compliance reporting is CQC-ready: dashboard views show training completion rates by training type, trainer, and time period.
The operational impact is substantial. AI-assisted training programmes reduce training compliance tracking time by 60-75% and achieve 95%+ compliance rates—compared to 70-80% typical of manual tracking. For CQC inspections, training compliance shifts from a risk area to a demonstrable strength.

Clinical Governance Integration and Risk Management Workflows
Healthcare organisations must weave together incident reporting, risk management, compliance monitoring, and corrective action tracking into a unified clinical governance framework. Historically, these were siloed: incident reports in NRLS, risk registers in spreadsheets, compliance audits in separate systems, corrective actions tracked ad hoc. Information did not flow between systems. A serious incident investigation might not reference the broader pattern of similar incidents. A compliance audit finding might not trigger a risk register entry.
AI-enabled clinical governance platforms integrate these silos. An incident is reported in NRLS. AI categorisation and clustering immediately identifies related incidents. A risk assessment algorithm assigns probability and impact. A risk register entry is auto-created. Corrective action workflows are instantiated. Clinical governance teams are notified with priority escalation. Root cause analysis is guided by AI suggestions. When root causes are documented, the system links back to the original incident, updating the risk register and informing future risk assessments.
For a trust, this integration means clinical governance becomes a data-driven, systematic discipline rather than a reactive, ad hoc process. Serious incident investigation times are reduced. Learning from incidents is systematically captured and disseminated. Risk registers reflect actual safety threats rather than historical lists.
Implementation Challenges: Change Management and Staff Adoption
The evidence for AI compliance benefits is compelling, yet adoption barriers remain substantial. Mid-market NHS trusts report insufficient vendor education and change management support as primary obstacles to implementation. Clinical staff fear that AI-driven incident categorisation may alter reporting patterns or create punitive consequences. Compliance teams accustomed to manual processes resist new systems. Data quality issues limit AI accuracy: if incident narratives are poorly structured, AI categorisation suffers.
Successful implementation requires more than technology. It demands change management, staff training, and cultural shift. Helium42 differentiates itself through education-led implementation: extensive staff training and change management support help compliance teams understand and trust AI outputs. This addresses a critical adoption barrier. Rather than imposing AI systems on unwilling teams, education-led implementation involves clinicians and compliance staff in the process, building confidence in AI recommendations through transparency and proven track record.
Healthcare organisations exploring AI implementation should prioritise vendors offering comprehensive change management, not merely technology. The best platform is useless if staff distrust it and revert to manual processes.
Return on Investment: Quantified Compliance Benefits
The financial case for AI compliance investment is strong. Time savings across compliance functions range from 40-75% depending on activity. For a 600-bed acute trust:
CQC inspection evidence gathering: 40-56% time reduction = 50-90 hours saved per inspection = £2,500-£4,500 labour cost savings per inspection cycle.
Monthly regulatory submissions: 50-62% time reduction = 20-40 hours saved per month = £1,000-£2,000 monthly saving = £12,000-£24,000 annualised.
Policy deviation audits: 60-75% time reduction = 40-60 hours saved per audit = £2,000-£3,000 per audit cycle.
Staff training compliance tracking: 60-75% time reduction = 15-30 hours saved per month = £750-£1,500 monthly = £9,000-£18,000 annualised.
Total annualised savings (time-related): £45,000-£80,000 for a mid-market trust, with larger trusts achieving proportionally higher absolute savings.
Beyond time savings, breach prevention and avoidance of regulatory penalties represent substantial value: a single significant breach of GDPR can result in fines of 2-4% of annual revenue; CQC-triggered enforcement action can impose substantial remediation costs and operational constraints. While quantifying breach prevention ROI requires assumptions about breach probability and severity, the insurance value of systematic compliance is evident.
Regulatory Guidance and Emerging AI Compliance Standards
Regulatory bodies are beginning to formalise expectations around AI use in healthcare compliance. The Care Quality Commission published exploratory guidance on AI monitoring and announced pilot programmes with NHS trusts, though specific mandate timelines remain undefined. The Information Commissioner's Office has issued guidance on AI and GDPR compliance, emphasising the importance of Data Protection Impact Assessments and documented lawful basis for AI processing of personal data. NICE (the National Institute for Health and Care Excellence) has published guidelines on AI safety and effectiveness evaluation in clinical contexts.
For healthcare organisations implementing healthcare AI solutions, alignment with these emerging standards is critical. Regulators expect organisations to demonstrate not just that they use AI, but that they have conducted rigorous compliance assessments, documented governance frameworks, and implemented controls to mitigate risks.
Healthcare Compliance AI: Frequently Asked Questions
What is the difference between AI-assisted compliance and fully automated compliance?
AI-assisted compliance systems augment human judgement; they do not replace it. An AI system might flag a policy deviation or suggest incident categorisation, but a compliance officer makes the final determination. Fully automated compliance (AI makes final decisions without human review) remains rare in healthcare due to regulatory and liability constraints. The best systems combine AI pattern detection and recommendation with human oversight and final decision authority.
How do AI compliance systems ensure they do not introduce bias or errors?
Bias in AI systems typically arises from training data. If historical incident reports are biased towards reporting incidents in certain wards or against certain staff, AI trained on that data will perpetuate bias. Responsible vendors implement bias testing, diverse training data, and explainability mechanisms. The system should be able to explain why it categorised an incident as "high risk" or why it detected a policy deviation. Organisations should demand independent validation of AI systems before deployment.
What data protection measures are necessary when implementing AI compliance systems?
AI compliance systems handle sensitive health and operational data. Organisations must conduct Data Protection Impact Assessments, establish appropriate data processing contracts with vendors, implement data minimisation (using only necessary data for compliance purposes), and ensure audit trails document all data access. Organisations should verify that vendors store data in the UK or secure EEA jurisdictions post-Brexit, with appropriate data transfer safeguards.
How long does it typically take to implement an AI compliance platform?
Implementation timelines vary by system complexity and organisational readiness. A compliance monitoring system integrated with existing IT infrastructure might deploy in 3-4 months. More complex implementations involving integration with multiple clinical systems, staff training, and change management can extend 6-9 months. Organisation should expect phased rollout: pilot in one department, validate, then expand organisation-wide.
Can smaller healthcare organisations afford AI compliance systems?
Smaller providers may find upfront costs challenging, but cloud-based SaaS platforms are reducing barriers. Organisations should evaluate total cost of ownership (including staff time reduction), seek vendor partnerships on phased implementation, and consider shared platforms offered by healthcare networks or ICBs. Some vendors offer risk-sharing arrangements: savings are shared between vendor and organisation.
Related Reading
Explore related articles in healthcare AI implementation and governance:
- AI for Healthcare: Transforming Patient Care and Operational Efficiency
- AI for Medical Imaging: Diagnostic Accuracy and Clinical Workflow Integration
- AI for Pharmacy: Medication Safety and Antimicrobial Stewardship
- AI Consultancy: Building Organisational AI Capability
- AI Training Programmes: Education-Led Implementation
- AI for Dentistry: Transforming Dental Diagnostics and Practice Management
- AI for Clinical Documentation: Automating Medical Records and Note-Taking
Ready to Strengthen Healthcare Compliance with AI?
Helium42 helps healthcare organisations build internal AI capability through education-led implementation. From CQC readiness to clinical governance, our programmes deliver measurable results in 6 to 8 weeks. Over 500 companies and 2,000+ healthcare professionals have engaged our training and consultancy services, achieving 95% satisfaction rates and typical efficiency gains of 40% across compliance operations.
Book a Consultation

